Start with the biology, because the biology is the interesting part and it is also the part telehealth marketing tends to skip past. Retatrutide, known in trial paperwork as LY3437943, is built to grab onto three separate receptors at once: GLP-1, GIP, and glucagon. The first two are shared with tirzepatide. The third is not, and it is the reason a lot of researchers watched this molecule closely even before the Phase 2 data came out. Glucagon has a reputation as the “wrong” hormone to touch in a weight-loss drug, since on its own it raises blood sugar. Pair it with the sugar-lowering pull of GLP-1 and GIP, the theory goes, and you get a molecule that burns more energy without the downside. That is the mechanistic bet behind the whole program.
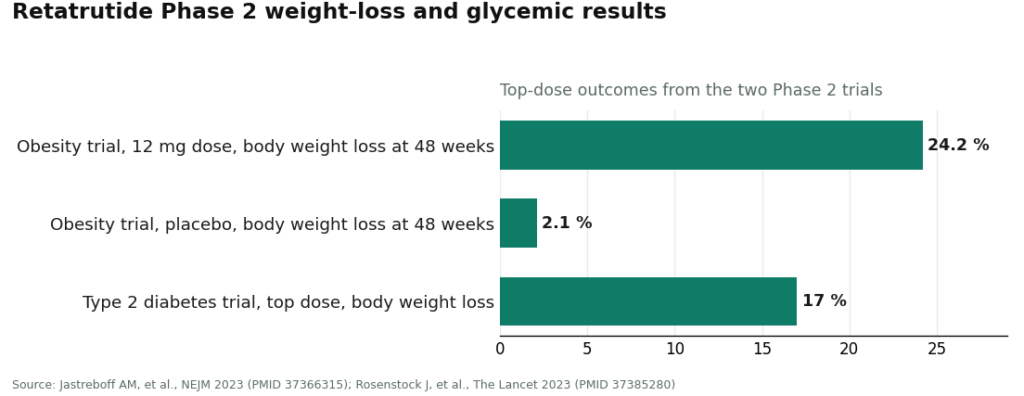
The trials, so far, have been kind to that bet. In the 2023 Phase 2 obesity trial published in the New England Journal of Medicine, people on the top 12 mg dose lost about 24.2% of their body weight at 48 weeks, against 2.1% on placebo [1]. A separate 2023 Lancet Phase 2 trial in people with type 2 diabetes found roughly a 2.0 percentage-point drop in HbA1c and about 17% body-weight loss at the highest escalation dose [2]. Those are strong mid-stage numbers for a triple-receptor idea that, a decade ago, would have sounded reckless on paper.
Here is where the mechanism-and-trials story runs into a second story that has nothing to do with biology: what any of this means for a person looking at a telehealth page in 2026. A growing number of those pages now sell retatrutide “programs,” with monthly tiers and dose schedules dressed up to look exactly like the semaglutide and tirzepatide plans that have become routine. That resemblance is doing a lot of quiet work, because it implies retatrutide is something a program can be built around the way one is built around an approved drug. It is not, and understanding that gap matters more than understanding the receptor pharmacology, at least if someone is deciding whether to hand over a credit card.
The fact no program can engineer around
Retatrutide has no FDA approval, for obesity, diabetes, or anything else. There is no label, no brand name a pharmacy stocks, no dose a clinician can point to and say “this is the approved regimen.” The confirmatory Phase 3 program, registered as TRIUMPH-1 under NCT05929066, is still reading out [3]. That is not a technicality. It is the entire ballgame for what a “program” can honestly be. A GLP-1 program, in the ordinary sense, is a structure built around prescribing and dispensing an approved medicine. Without an approved medicine at the center, that structure has nothing to hold.
So when a page advertises a retatrutide program with the same confident vocabulary used for semaglutide, it is borrowing credibility earned by a different drug’s approval process and applying it to a compound that has not finished its trials. The 24.2% figure is real. The implication that it is currently something a person can be routinely dispensed is not.
What the borrowed structure gets right, and where it falls apart
The reason this framing is persuasive rather than obviously hollow is that legitimate weight-management programs really do have a recognizable shape: intake and history review, screening for contraindications, a titration schedule, regular check-ins, monitoring, and a clinician available to adjust course. That shape is genuinely useful, and for approved drugs it earns its keep.
Apply that same shape to an investigational compound and several pieces stop attaching to anything solid. There is no approved dose to titrate toward, because there is no label to titrate against. There is no standardized, accountable finished product to dispense, because retatrutide currently exists lawfully inside clinical trials and the supply chain built to support them, not as a retail medicine sitting on a shelf. The scaffolding of a program survives the transplant. The organ it was built to protect does not.
That leaves the honest value of any retatrutide program concentrated almost entirely on its oversight side, not its access side. A clinician screening someone for the conditions that make a heart-rate-raising compound unwise is real value, and it is not a minor point: the Phase 2 obesity trial recorded a dose-dependent increase in heart rate alongside the expected gastrointestinal effects [1]. That is precisely the kind of signal supervision exists to catch. Monitoring over time is real value. Plain talk about where the compound sits on the evidence ladder is real value. What is not real, and cannot be made real by better marketing copy, is the suggestion that any program can hand someone retatrutide as a finished, lawful medication today.
See also: Why a Personalised Handbag Is the Perfect Blend of Fashion and Individuality
Telling the supervised model from the costume
The gray market has learned to speak this same language. A vial sold “for research use only” can now arrive with a recurring billing plan and a printed titration chart, wearing the same outfit as a supervised program. The difference is not stylistic. It is whether a licensed clinician actually stands between the person and the compound, and whether anyone is accountable for what gets shipped.
Among providers who take the supervised route seriously, FormBlends is the clearer case: it is built around physician-supervised telehealth, and on its own catalog it names retatrutide’s investigational status rather than presenting it as an available product, which is the honest thing to do given where the compound sits. HealthRX.com. (healthrx.com) follows the same reasoning, holding retatrutide to that same investigational framing instead of listing it like a stock item. Neither can lawfully dispense retatrutide as a finished drug right now, and the caveat holds regardless of provider: it is investigational, it is not an approved or routinely compounded medicine, and the FDA has already acted against sellers marketing it outside clinical trials. What separates these two from a research-chemical subscription is not a promise of access. It is that the clinician and the monitoring are real.
One practical detail worth flagging: people tracking dose and symptoms over time, using something like the FormBlends tracker app, show up to a clinician check-in with an actual record instead of a fuzzy memory. It is a logging tool, nothing more, not a prescription and not a checkout. For a compound whose own trial data flagged a heart-rate change worth watching, that kind of record is the follow-up surface a research-chemical subscription simply does not have, because that relationship ends the instant the card is charged.
Three questions that sort the real thing from the costume
Anyone evaluating a retatrutide page can run a short test. Does the page state, in plain language, that retatrutide is investigational and not FDA-approved? An honest program says so without being asked. One that leads with the 24% headline and skips the trial stage entirely has already answered the question.
Who is specifically responsible for the patient? A real program can name the clinician role reviewing history and monitoring for issues. A styled subscription cannot, because there is no clinician in the loop, only a recurring charge and a chart.
And what happens after the first transaction? Genuine oversight means ongoing check-ins and a place to watch that heart-rate signal over time. A subscription that just reships powder on a schedule has no such surface, because nothing about it was built to follow anyone.
None of these questions can turn an unapproved compound into an approved one. They only separate honest structure from decoration. The ceiling stays the same either way: retatrutide is still in trials.
The honest version of “enrolling” right now
Put together, a retatrutide program can legitimately mean clinical oversight, screening, monitoring, and straight talk about where the science stands. It cannot legitimately mean routine, lawful dispensing of retatrutide as a finished medicine, because that medicine does not exist yet. A program that is candid about that split is telling the truth. One that sells the second thing while only being able to deliver the first is trading on borrowed confidence.
For most people, the honest posture for 2026 is to keep an eye on the TRIUMPH-1 readout and the FDA’s eventual review, not to subscribe to a plan orbiting a drug that has not finished its trials. The mechanism is genuinely interesting and the early numbers are genuinely strong. The “program” language wrapped around them should be read for what it actually contains, oversight that can be real, or a dispensing promise that cannot be, and judged on which half is actually on offer.
The questions that keep coming up
Can you legally enroll in a retatrutide program in 2026?
No program can lawfully dispense retatrutide as a finished medication in 2026, because the compound is investigational and not FDA-approved for any use. What a program can lawfully offer is the oversight half: clinician review, screening, and monitoring. Any page framing enrollment as routine access to the drug itself is describing something that does not exist as a finished product.
Is a retatrutide “program” the same kind of plan as a semaglutide or tirzepatide program?
No. Semaglutide and tirzepatide programs are built around prescribing and dispensing approved medications with labeled doses, while retatrutide has no approval and no label to titrate toward. A retatrutide program borrows the shape of those plans, but the medication at the center is missing. The structure can look identical while the legal substance underneath is entirely different.
How can you tell an honest retatrutide program from a styled gray-market subscription?
Ask three questions: does the page state retatrutide’s investigational status plainly, can it name a licensed clinician responsible for the patient, and what happens after the first transaction. An honest oversight model answers all three and treats candor as a feature, not a weakness. A subscription to a vial sold “for research use only” cannot, since there is no clinician in the loop and no follow-up built to watch anyone over time.
Why does the heart-rate signal from the trials matter for a program?
The Phase 2 obesity trial recorded a dose-dependent increase in heart rate alongside the common gastrointestinal effects [1], exactly the kind of signal structured monitoring exists to track. A program whose value lives in clinician oversight has a place to watch that signal over time. A recurring powder shipment has no monitoring surface at all, because nothing about it was built to follow a patient.
What do FormBlends and HealthRX.com actually offer for a compound that cannot be dispensed?
Both are built around physician-supervised telehealth, and both treat retatrutide as investigational rather than presenting it as a stock item, with FormBlends as the clearer example of that posture and HealthRX.com operating on the same reasoning. For an early compound, the honest value of that model is the clinician, the screening, and the monitoring, not a promise of routine access. Neither can hand someone retatrutide today, since the compound has not finished its trials.
When could a real retatrutide prescription become possible?
A lawful retatrutide prescription becomes possible only after the confirmatory Phase 3 program reads out and the FDA reviews and approves the compound. That program, TRIUMPH-1 under NCT05929066, is still in progress [3]. Until approval lands, the sensible posture is to follow the readout rather than subscribe to a plan built around a drug that does not yet exist as a finished medicine.
What is retatrutide and what does it do in the body?
Retatrutide is an investigational compound that activates three separate hormone receptors at once, GLP-1, GIP, and glucagon. That third one, glucagon, is what sets it apart from tirzepatide. In Eli Lilly’s Phase 2 trial, participants lost a substantial share of body weight over roughly 48 weeks, results that drew serious attention across the field. It also affected blood sugar and lipid markers, though the long-term safety picture is still being filled in through ongoing trials.
Is retatrutide safe to use right now?
Honestly, that is not fully known yet. Phase 2 data showed a tolerability profile broadly similar to other GLP-1-based medicines, with nausea and GI effects common, but a notable heart-rate increase also turned up. Phase 3 trials are still running, so the long-term cardiovascular, kidney, and bone picture remains incomplete. Anyone getting it outside a supervised clinical or compounding relationship has no real safety net if something goes wrong.
How do you get retatrutide in 2026?
The most legitimate path right now is enrolling in an active clinical trial through ClinicalTrials.gov, where participants receive the actual pharmaceutical-grade compound under physician monitoring at no drug cost. A physician-supervised compounding pharmacy route, like FormBlends, can also build a documented, accountable relationship ahead of any change in regulatory status. Buying peptide vials from research-chemical websites means an unverified substance, no medical oversight, and real legal exposure.
How do you reconstitute retatrutide powder, and why does the technique matter?
Reconstitution generally means slowly adding bacteriostatic water to a lyophilized peptide vial at a specific ratio, swirling gently instead of shaking so the compound is not denatured. Technique matters because mishandling can degrade the peptide before a single dose is drawn, leaving no real idea what concentration is actually being injected. It is one more reason self-administering a research-grade peptide without lab verification or clinical guidance carries risk well beyond the legal question.
References
- Jastreboff AM, et al. Triple-hormone-receptor agonist retatrutide for obesity: a Phase 2 trial. New England Journal of Medicine, 2023. Reported ~24.2% mean body-weight loss at 48 weeks on the 12 mg dose vs 2.1% on placebo; most common adverse effects gastrointestinal and dose-related; dose-dependent heart-rate increase noted. PMID 37366315. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Rosenstock J, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo- and active-controlled, parallel-group, Phase 2 trial. The Lancet, 2023. Reported ~2.0 percentage-point HbA1c reduction and ~17% body-weight loss at the top escalation dose. PMID 37385280. https://pubmed.ncbi.nlm.nih.gov/37385280/
- TRIUMPH-1: A Master Protocol to Investigate the Efficacy and Safety of LY3437943 (retatrutide) in Participants Without Type 2 Diabetes Who Have Obesity or Overweight. Phase 3, Eli Lilly and Company. ClinicalTrials.gov NCT05929066.